Well what do you think? Is it? It may well depend who you are. If you are a GP you are unlikely to think so, but as a hospital Chief Executive, who has heard all about the workload and workforce pressures general practice is under, it is easy to draw the alternative conclusion.
But correlation, as my PhD wife constantly reminds me, is not the same as causation. The fact that general practice is struggling with workload pressure at the same time as there is rising demand in A&E only means the two are correlated. It doesn’t necessarily mean one causes the other. And so it is that research was published this week in the British Journal of General Practice looking at the factors affecting emergency department attendance. They found (drum roll),
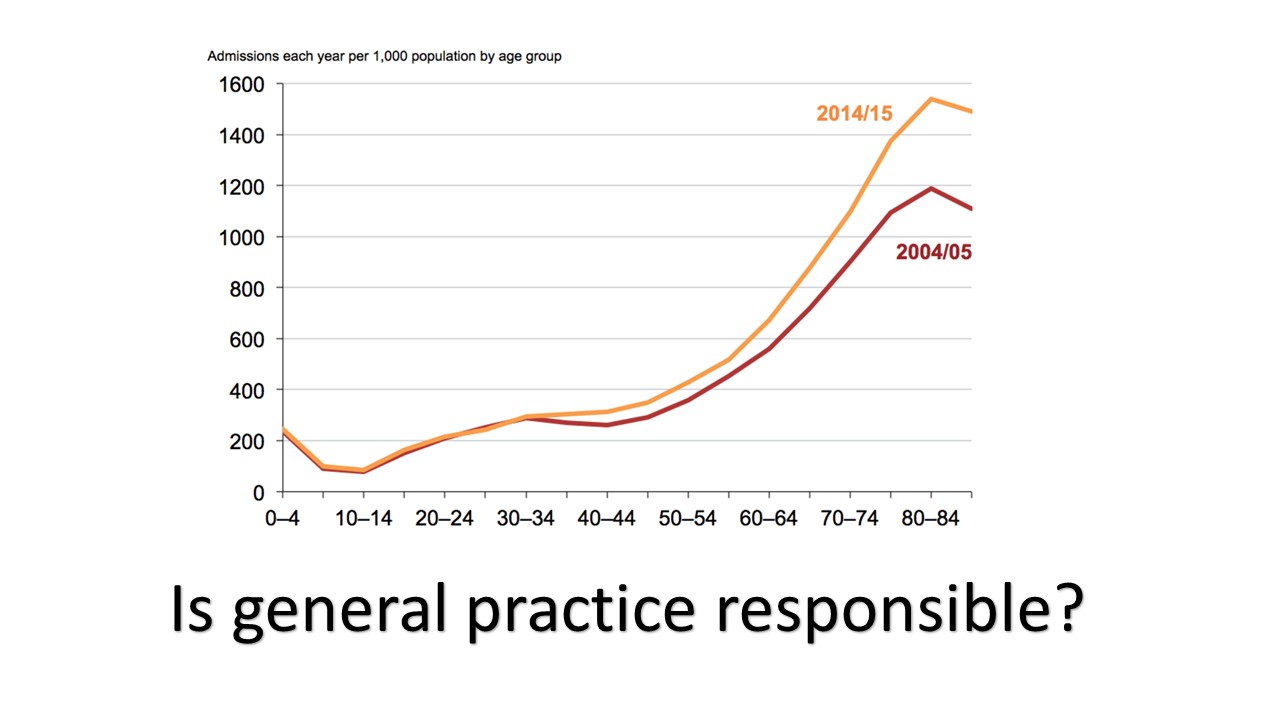
“…the burden of multimorbidity is the strongest clinical predictor of ED attendance, which is independently associated with social deprivation. Low use of the GP surgery is associated with low attendance at ED. Unlike other studies, the authors found that adult patient experience of GP access, reported at practice level, did not predict use.”
In other words, people are living longer with more long term conditions. This in turn is causing the growth in demand, both for GP practices and A&E departments. The more GP consultations a person has, the more likely (for many groups) it is that they will also have more A&E attendances. Growing demand is the causative factor. Pressure on A&E departments and GP practices are simply correlated.
I am on Twitter (@BenXGowland – the X is actually my middle initial, as opposed to denoting membership of some secret society). You should be too. The GP I most enjoy following on Twitter is Dr Steve Kell (@SteveKellGP). He recently ran a survey (now I recognise I need to be careful here as having preached about the difference between correlation and causation, I know I am going to get stung on the validity of a small sample size, but nevertheless) which found that, of the 48(!) GP practices that responded, 81% had not been asked if they were busy or managing in the first week of the New Year, with only 19% saying that they had. Steve’s concern is that “sadly we value what we measure”.
But simply knowing that a problem exists (there is too much demand, and it is getting worse) does not actually help. Nor does finding someone to blame (whether it is GPs blaming hospitals, or vice versa, or the government, or Jeremy Hunt etc etc). The only real option is to work out what we can do about it (because even if there was more money, which there isn’t, there will never be enough).
Which brings me to another interesting exchange on Twitter involving my friend Dr Kell. His practice is a leading light in the Primary Care Home movement, and he announced on Twitter that his practice had achieved a (highly impressive) 5.5% year on year reduction in emergency admissions. Now that prompted a question in response from Professor Harris of Lakeside Health asking,
“where lies the incentive (other than patient benefit) of GPs working harder/differently/more productively if the £ benefits remain with trusts or CCGs?”
The essence of this question is what is the point of the primary care home, of groups of practices working with other agencies, and managing demand in a different way in the way that Dr Kell’s practice has, if there is no financial return for the practice? His response was that while there is no direct financial return, it makes things better for patients, for staff, and is more efficient.
If we think about this in the context of constantly rising demand, the challenge practices face is how to adapt to meet this demand in different ways. Not because there is a direct and immediate financial benefit, but because the current system is not working, and without change the system is likely to collapse. Everyone working in the system has a responsibility to understand and accept the current realities, and to think and act differently as a result, so that things can improve.
General practice is not responsible for the pressures A&E is experiencing, but it is responsible for adapting and finding new ways of dealing with the demand (like the work being undertaken within the primary care home sites) so that general practice, and the NHS, can continue to manage the rising burden of disease. And if you take nothing else away from this, at the very least you should follow @SteveKellGP on twitter…

No Comments