One of the problems I have been grappling with in recent weeks is trying to work out why there is no single, universally applicable model of governance that GP federations can adopt. I have seen governance models that have worked really well in one area be a real hindrance to progress in another, and I wanted to understand why.
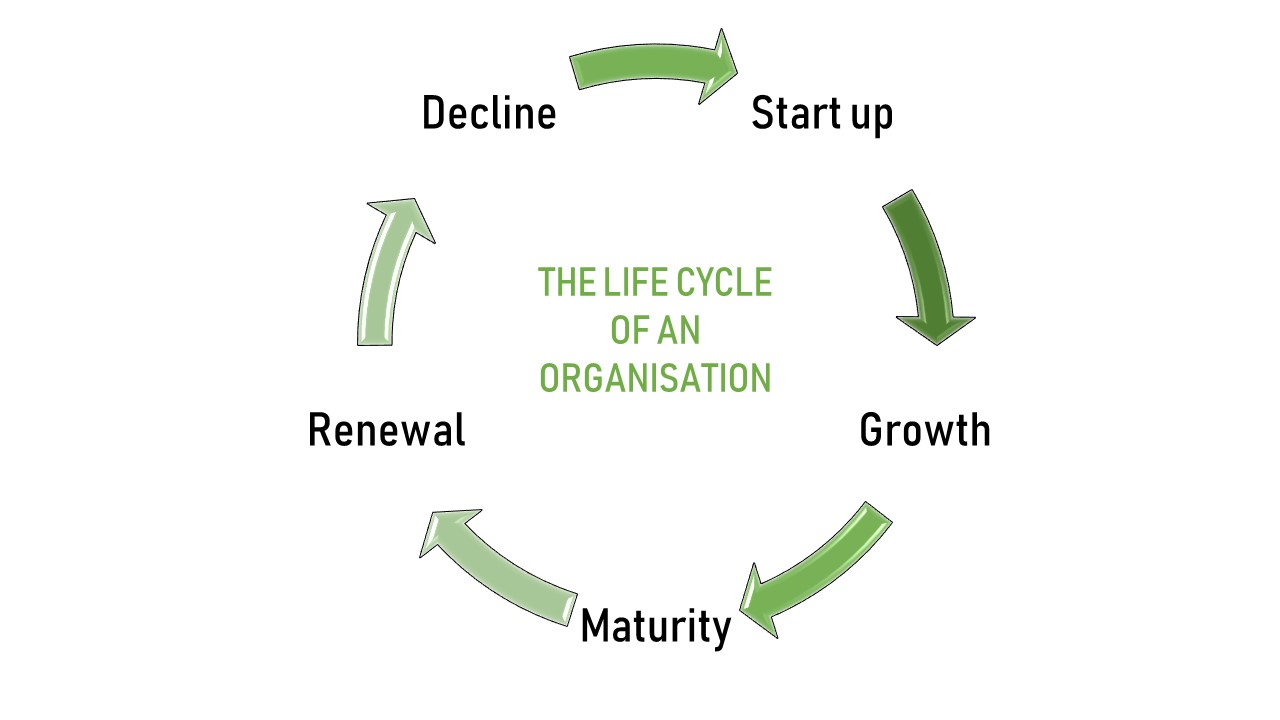
What has helped me unpick this is thinking about organisational life cycles. If you are not familiar with these, essentially each organisation goes through a life cycle from creation through to termination. People who look at these things have found organisations do not progress through a series of random events, but rather through an expected sequence of stages. These are start-up, growth, maturity, renewal and decline[i].
Different organisations go through these stages at different rates. Some companies like Blockbuster Video and Boo.com (anyone?) came and progressed quickly through to decline, while others like Colgate and Cadburys feel like they have been around longer than most of us can remember. Some, of course, never make it out of the start-up phase.
This helps us understand why the ‘cut and paste’ model of federation governance doesn’t work because the governance needs of an organisation vary according to the stage of development it is at. In a start-up it is generally all hands on deck with everyone (including the board) doing what is needed to get the idea off the ground. During the growth phase the board is more focussed on plans and policies. And as the organisation gets to maturity the focus of the board is much more on strategy, risk management and holding the leader/CEO to account.
This means asking “what is the correct governance for a GP federation?” is actually the wrong question. The right question is “what stage in its organisational life cycle is the GP federation at?” Once that has been established, we can match the appropriate governance to it.
The trap I see many GP federations falling into is failing to match the appropriate governance with where they are in the organisational life cycle. In particular, many GP federations are in start-up – they have developed a shared vision/mission across the member practices, and there are a small number of leaders trying to maintain engagement and enthusiasm while at the same time getting projects off the ground to prove the worth and value of the organisation. But they spend their time investing in lawyers and developing complex governance arrangements that are appropriate for a more mature organisation.
It is hard enough being a start-up organisation. There are so few people trying to do so much, at the same time as having sceptics to convince. The precious limited resource that is the time and energy of the leaders needs to focus initially on getting ideas off the ground and turning them into action, and of convincing stakeholders that this really is the future. Spending it on creating overly complex governance structures at this stage diverts energy from where it is really needed (as well as being expensive!).
Meanwhile, the high performing federations have already been through the start-up stage. They may even have gone through rapid growth. So the governance they now have is of a mature organisation (looking at strategy, risk management and holding the leaders to account). This is appropriate for them now. But it wasn’t appropriate when they started, and simply because you aspire to be like them doesn’t mean that it is appropriate for your organisation now either.
There is no single perfect governance model for a GP federation. But being clear on where your federation is on its organisational life cycle is the best first step you can take to determine what the most appropriate form of governance is for you.
[i] Lester, D., Parnell, J. and Carraher, S. (2003). Organizational life cycle: A five-stage empirical scale. International Journal of Organizational Analysis, 11(4), p.339-354



