This is the third in a five-part series of blogs discussing the independence of general practice. This week Ben looks to the Nigel Watson-led review of the partnership model and considers the possible threats this poses to that independence.
Why the review of the GP partnership model makes me nervous
In February Jeremy Hunt announced there would be a review of the partnership model of general practice, and that it would consider “how the partnership model needs to evolve in the modern NHS”. This review makes me nervous.
The number of GP partners is falling. As all practices are only too well aware, the number of applicants for a GP partner post has fallen dramatically, with many adverts not attracting a single serious application. General practice has to be attractive to the GPs of the future. The review will need to look into this, and discover nuggets such as “the prospect of unlimited personal liability in a hugely under-funded sector has limited appeal to new GPs”.
I am nervous about this review because it is very easy to conflate the issues facing general practice as a whole (the workload, workforce and financial pressures) with the partnership model. It is easy to imply it is the partnership model causing the challenges rather than the historic underfunding etc. etc. Correlation, regular readers of this blog will recall, is not the same as causation. If general practice was still receiving 11% of NHS expenditure would we still be having this review?
A review of the partnership model is also a review of independent contractor status. General practice is currently very difficult to control. The independent contractor status affords it an ability to act only according to what is negotiated within its contract. Changes to NHS rules don’t directly affect it. Persuasion rather than coercion is required, and for politicians seeking rapid change in general practice I can imagine this is hugely frustrating.
There is a widely-espoused view that the small business, or “corner shop” model of general practice is no longer fit for purpose. As the NHS seeks to move into a world of integrated care a new, bigger version of general practice is required that can partner with the rest of the system. Most sectors of the NHS can be instructed to actively participate in integrated care arrangements (or individuals moved on), but not so general practice. The sheer number of practices is making progress painfully slow, and there is no direct command lever that can be pulled to make integration happen any faster.
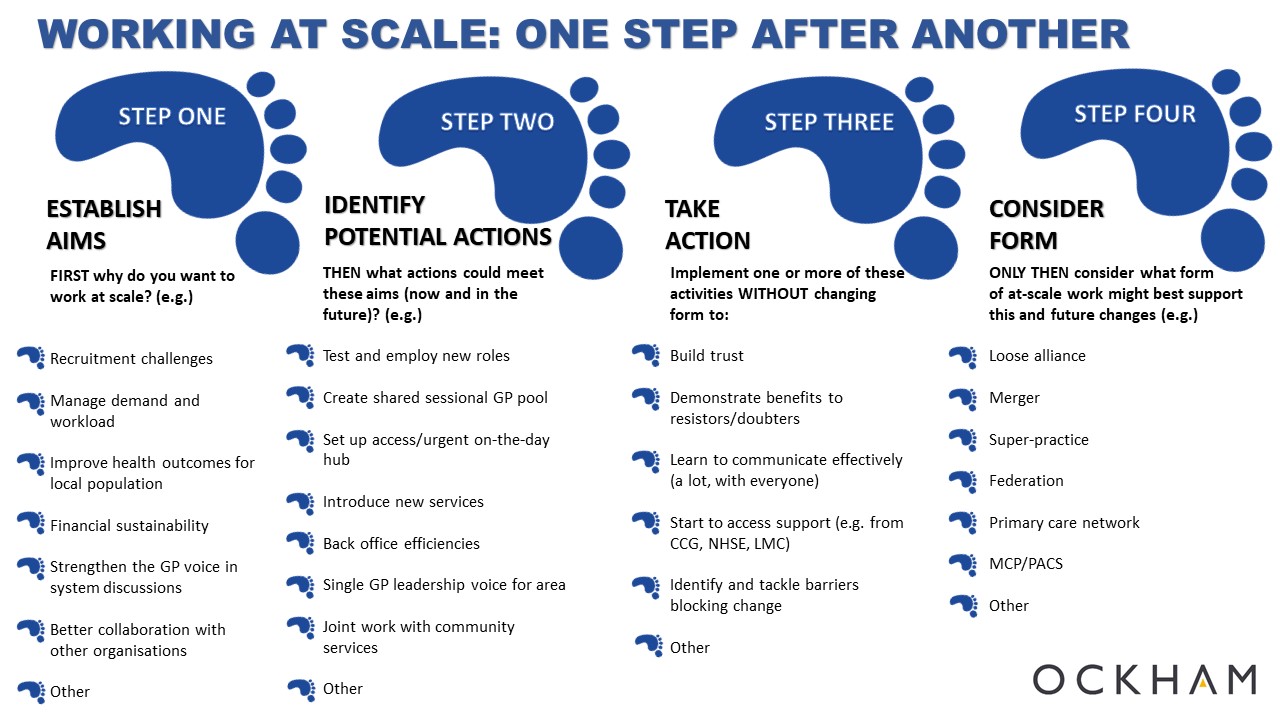
However, size and form are two different things. GP partnerships, operating as independent contractors, can operate at any scale. They are not limited in size. Our Health Partnership has done an admirable job of demonstrating how the partnership model can work at a population scale of over 300,000. Conflating the relatively small size of general practice organisations with the partnership model of general practice when they are two distinct issues is, at best, unhelpful.
The review makes me nervous because although the partnership model does not need to change for general practice to operate at greater scale, it does need to change if the system is to exercise greater control over general practice.
The only thing making me less nervous about the review is the appointment of Dr Nigel Watson, Chair of Wessex LMC to lead it. He appears to be a supporter of the partnership model. He recently said,
“My personal view is that the partnership model has not reached the end of the road, it can still have an important role to play in the future of the NHS but we need to make it a better place to work, which will encourage more GPs to remain working in general practice, address the concerns about the unlimited personal liability and with the move to a more population based approach to healthcare ensure that general practice is truly able to play a leadership role in the local NHS.”
The review does indeed need to consider these things, and build on the strengths and freedoms of the partnership model as it looks to the future. Let’s hope my nervousness (and, I admit, my cynicism) is unfounded.