When I was about 5 years old my brother and I became supporters of Liverpool Football Club. No-one told us we had to. Our parents were not football fans. We did not have to sit in a class to learn about Liverpool Football Club, or pass an exam before we could watch them play. No-one forced us to learn the names of all the players, or their shirt numbers, or the endless statistics from the previous decade. We learnt about the club because we were passionate about it which created our energy and enthusiasm to find out as much as we could, whenever we could, and to pester our father constantly to take us to matches.
Whilst not a football fan, my mother was a catholic. So when we were the same age every Sunday she used to make me and my brothers go to church. We never asked to go, and we went because we had to. We didn’t pay attention, got out of going whenever we could, and spent our time when we were there daydreaming about Anfield and whether Liverpool would win when they next played, as well as generally causing trouble. Eventually, we made life so miserable for my mother that she stopped making us go.
Now I am older, things are not much different. I spend my time doing the things I am passionate about and enjoy doing. There are some things I have to do (chores, shopping etc.), but, as my wife will no doubt attest, I do them as quickly as I can (or try and get out of them!) so that I can focus my efforts on the things that matter to me.
My brother is the same. In fact, we all are. We all want to spend time doing the things we want to do and care about, and avoid doing things we are doing because we have to. GPs are no different. Most GPs want to spend their time in the practice, focussing on making a difference to patients and the things that matter, not doing the things they feel they have to do (but hate) like preparing for a CQC inspection, or attending yet another CCG meeting.
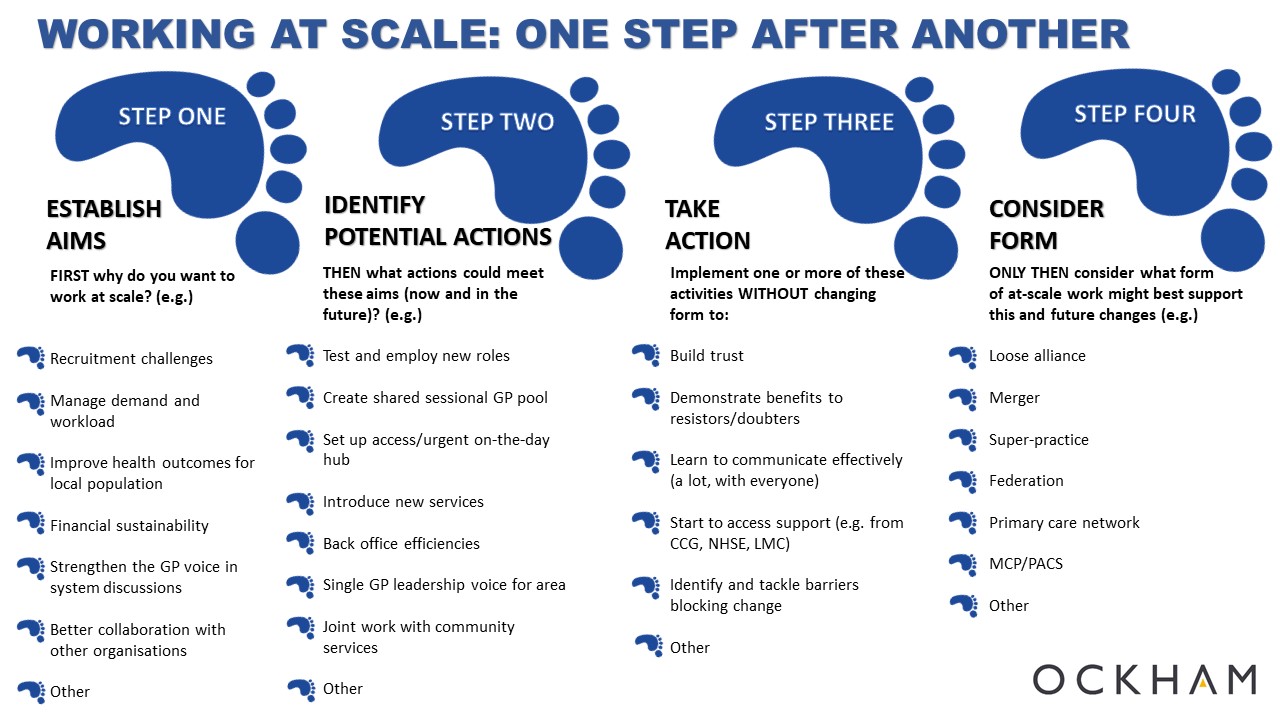
For GPs, where does operating at scale fit in to the spectrum, where “doing it because we have to” is at one end, and “doing it because we are passionate about it and the difference it can make” is at the other?
Looking around the country, it varies.
Some GPs are really passionate about operating at scale. They believe it is key to the sustained future of the profession, to ensuring GPs have a strong voice around the system table and to giving them the best chance of making a difference to the lives of their patients. They seemingly work 24 hours a day on making it happen, putting all their spare time into it, and do so with boundless energy.
But many GPs are doing it because they feel they have to. They feel the weight of system pressure pushing them in that direction, and go along with it because even if they recognise there is some logic to it, their heart is in small, independent general practice. Unsurprisingly, they rarely turn up to meetings, they contribute only what they have to, and are often negative and disruptive.
GPs working at scale because they want to, not because they have to, is what will create the energy to make something great happen. It is what already differentiates those really successful examples of working at scale from the rest. Getting the majority of your colleagues to agree to doing something they do not believe in is storing up problems for the future. Jumping into a federation or a network without even knowing why is a mistake, because you won’t invest of yourself in it.
Spend time on why. Spend as much time as it takes to generate energy for a movement, and only then move forward. That investment of time will repay itself multiple times in the future, because it won’t feel like (your equivalent of) going to church, but instead like going to Anfield!